






 Si no encuentras el que quieres nosotros te lo buscamos
Si no encuentras el que quieres nosotros te lo buscamos 9:58
9:58
 Daniel Enriquez de Guevara
Daniel Enriquez de Guevara
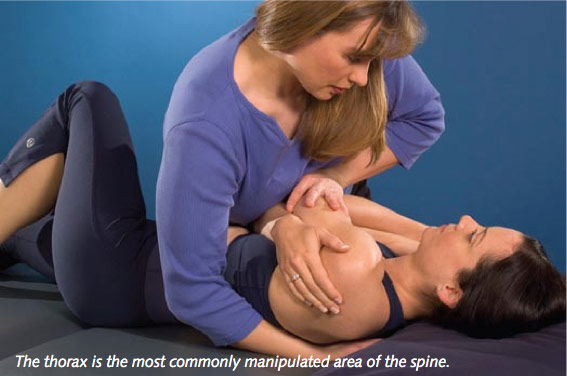
IS IT TIME FOR A CLOSER LOOK AT THE THORAX?
This article was written by Linda-Joy Lee (BSc, BSc (PT), FCAMT, CGIMS, MCPA), a Canadian Institutes of Health Research (CIHR) Fellow, clinical physiotherapist, and educator. She is known internationally for her skills in movement and performance analysis to restore optimum function and her integrated approach to treatment. We are very appreciative of her permission to reprint this article. The article originally appeared in In Touch journal, an official publication of Physio First.
Many clinicians recognise that the thorax is an important area to assess and treat, not only in patients with thoracic pain and dysfunction, but also in patients with lumbopelvic and cervical pain (McConnell 2005; Lee & Lee 2004; Butler 1994). The thorax is an important region of force transmission in the body, transferring loads between the legs and lumbopelvic region, and the arms, neck and head (Singer & Edmondston 2000). It is also a central area of myofascial connections; a large number of muscles that control the head, neck, shoulder girdle, and lumbopelvic region have their origins in the thorax. Furthermore, the thorax functions as a protective unit for the heart and lungs and facilitates optimal respiratory function, as well as being closely related to the autonomic nervous system.
In order to understand the role of the thorax in transferring load for optimal function, pain is not the only factor to consider. The stiff, pain-free thorax, much like the stiff, pain-free hip, can create excessive loading and mobility demands in adjacent areas, resulting in excessive movement, compression, shear and/or tensile forces, irritation and eventually pain. McConnell (2005) noted that, 'Many patients with chronic low back pain have associated stiffness in the thoracic spine... Increasing the mobility of the thoracic spine and the surrounding tissues will allow a more even distribution of load through the spine during movement.' Clinical observations suggest that the same is true of patients with cervical pain, and some researchers have started to investigate the impact of treating the thoracic spine in patients with neck pain (Cleland et al. 2005).
Treatment techniques for the thorax are most commonly directed towards increasing mobility of the thoracic spine. Techniques used include mobilisation, manipulation, soft tissue and myofascial release techniques, muscle energy, and dry needling. Indeed, in a survey of UK manual therapists, the thoracic spine was the area of the spine most frequently manipulated (Adams & Sim 1998). From a clinical perspective, these techniques change mobility of the thorax, at least in the short term, and create more optimal load sharing throughout the spine. exercise approaches are also designed around increasing mobility of the thorax (foam rolling, rotational stretches), but in terms of muscle training, common approaches focus on postural control, scapular control, dissociation of the thorax from the scapula/arms/ pelvis, and on training co-contraction of the global trunk stabilisers (erector spinae and superficial abdominals) (Lee DG 1994; Hall & Brody 1999; sahrmann 2001).
Seated rotation exercise for maintaining thoracic mobility.

It is interesting to consider the question: 'Is 'stiffness' the only problem with the thorax?' True joint fibrosis, unless there is a continuing underlying pathological process (such as in AKs), is treatable with sustained grade IV mobilisation techniques within 2-3 sessions (Lee DG 2003). Therapists most commonly use oscillatory mobilisations and manipulation to treat what they feel is a 'stiff thorax'; however, neither of these techniques are effective when the underlying impairment is true articular fibrosis. And why is it such a common experience for therapists and patients alike to have to repeatedly perform release, mobilisation and manipulation of the thorax?
It is a commonly held view that the thorax is inherently stable and inherently stiff due to the presence of the ribcage. While it is true that the presence of the ribcage affords more passive stability to the thoracic spine than the neighbouring cervical and lumbar regions, the ribcage itself is not a solid block of bones. A typical thoracic segment, which we define as the 'thoracic ring', has 13 articulations per ring, and in total the thorax contains 136 joints. each of these joints has the capacity to move in multiple planes, and where there is movement, there are requirements for motion control. Consider that, in terms of range of motion for trunk rotation, the thorax provides the majority of movement, with 6-9 degrees of movement (in one direction) per segment (White & Panjabi 1990) as compared to only 2-3 degrees of rotation available per lumbar segment (Bogduk 1997). The thorax is the centre for rotation of the trunk, essential for the production, modulation, and transmission of rotational torques. Thus, rotational control in the thorax is critical for optimal function. Consider many activities of daily living, and sports activities such as throwing, kicking, and running-they require not only control of inter-regional rotational control between the thorax and pelvis, but also inter-segmental control of rotation within the thorax.
Thus, the neuromuscular requirements for control in the thorax are the same as have been described in other regions of the spine-intersegmental, inter-regional, and postural equilibrium (Hodges 2003), but due to the complexity of the articulations, one additional category can be added. If we define the typical 'thoracic ring' as consisting of two adjacent vertebrae and the intervening intervertebral disc, the right and left ribs attaching between the two vertebrae, and the anterior attachments to the sternum, optimal function of the thorax requires 'intra-ring' control between the joints within the ring, 'inter-ring' control (intersegmental) between rings, inter-regional control (between the thorax and pelvis, thorax and head, thorax and shoulder girdle) and control of postural equilibrium. Control of movement is provided by appropriate activation, sequencing and modulation of force in the myofascial system, which is governed by the neural control system.
Specific thoracic ring palpation during trunk rotation task (Lee, LJ 2003).

Clinical observations indicate that patients can present with non-optimal strategies for control of the thorax, both segmentally and multisegmentally. The direction of poor control is usually into rotation, but can also be into posterior or anterior translation, although this is less common in the thorax than in the lumbar or cervical spines. The biomechanics of rotation as proposed by DG Lee (1993) outline that when rotation occurs segmentally in the thorax, a contralateral translation also occurs. This can be palpated laterally on the ribcage, on several rings simultaneously, during rotation of the trunk as well as during tasks that require rotational control (Lee LJ 2003). In patients with non-optimal strategies in the thorax, specific rings can be felt to: (a) not move into the contralateral translation (usually consistent with the vertebral component not rotating), (b) move excessively into the contralateral translation, or (c) translate ipsilaterally (the incorrect direction). All of these are examples of failed load transfer during the task of thoracic rotation.
Options (a) and (c), you may say, are just new ways of describing the 'stiff' thorax-the segment is not moving optimally. However, often these patterns are paired with observations of the same segment (ring) moving or moving excessively during tasks where there should be no intersegmental movement (failed load transfer for the task).
For example, the Prone Arm Lift (PAL) and the sitting Arm Lift (SAL) have been proposed (Lee, LJ 2003; Lee, LJ 2005) as clinical tests to detect loss of inter-ring control in the thorax. In the SAL, upon initiation of lifting the arm into flexion, the thorax should provide a stable base, and no shifts or translations should occur in any direction intersegmentally in the thorax. In patients with non-optimal strategies for control in the thorax, specific rings can be felt to translate, usually laterally, indicating lack of rotational control at those specific segments. These same rings display non-optimal biomechanics during trunk rotation. Clinical reasoning suggests that a ring that (a) doesn't move during trunk rotation, but (b) shifts laterally during the SAL cannot truly be 'stiff'.
Specific thoracic ring palpation during the SAL (Lee, LJ 2005).

It is proposed that these patterns are explained by altered timing and recruitment between the long superficial muscles of the thorax (for example, thoracic longissimus, thoracic iliocostalis) and the deep segmental muscles that are hypothesised to control intra-and inter-ring control, namely the thoracic multifidus, the intercostals, the levator costarum, and the diaphragm. There is some early scientific evidence to support this; subjects without spinal pain exhibit a pattern of decreasing activity in the contralateral longissimus during trunk rotation (Lee, LJ et al. 2005) and clinically we can palpate increasing activity in the contralateral longissimus in subgroups of patients with non- optimal control strategies in the thorax. The deep multifidus and superficial longissimus have also shown to be differentially active during fast arm movements during perturbations to the trunk requiring rotational control (Lee, LJ et al. 2007).
Other clinical observations are consistent with this hypothesis. At the ring levels of non- optimal control, palpable changes in resting tone of segmental multifidus and the intercostals can be felt, and interventions to train isolated recruitment of these segmental muscles (using imagery, touch and ultrasound feedback) and then integrate this recruitment into tasks requiring rotational control (Lee, LJ 2003) yield good clinical outcomes. Interestingly, when this approach is used, patients who have had or feel the need for repeated ongoing release and manipulation of the thorax then report that they no longer have that need or feel the 'stiffness' in their back.
So, maybe the 'stiffness' we feel, at least in a proportion of our patients, is not truly articular in nature, but rather, a reflection of the increased resting tone and dominance of the global muscles of the thorax (which also connect to the scapula, humerus, lumbopelvis, and neck) that creates neuromyofascial compression of joints of the thorax. The long global muscles do have specific fascicles of attachment that can impact one ring more than others due to segmental facilitation. This would explain why oscillatory mobilisations are so effective at treating this type of 'stiffness', as it changes the afferent input and through neurophysiological mechanisms could change the tone in muscles supplied by the segment. However, these techniques provide temporary change, and unless the inter-ring and segmental control are retrained and restored into movement strategies for function and performance, the 'stiffness' will return, and require treatment again. In non- optimal strategies for thoracic control, we see patterns of dominance or hypertonicity in several global muscles, paired with lack of recruitment in the deep local muscles specific to certain rings where there is lack of control. similar scenarios have been described and researched in the low back, pelvis and cervical spine, and clinical observations suggest that the same mechanisms can occur in the thorax as well.
Segmental palpation of thoracic multifidus at levels of non-optimal biomechanics often reveals atrophy or decreased resting tone. Lack of recruitment at these same levels can be palpated during specific tasks. Specific training can address these deficits.

How does this relate to other regions of the body? Let's consider just the relationships to the lumbopelvic region. Adaptations we have made to the Active straight Leg Raise (AsLR) indicate that poor inter-ring control can impact lumbopelvic control (Lee & Lee 2005).
In these cases, specific palpation of thoracic rings reveals that the segmental ring shift (usually the same as identified on previous tests) occurs at the initiation of lifting the leg of the side of the positive AsLR. When poor inter-ring control is contributing to the loss of lumbopelvic control, manual correction and stabilisation of the shifting ring causes the biggest change in ease of lifting the leg, even when compared to compressions across the pelvis. In these patients, assessment and treatment of the thorax seem to yield the best clinical outcomes as compared to a more local lumbopelvic treatment approach. Anatomical relationships can provide a rationale for these observations; however, there are likely multiple mechanisms at play. Conversely, there are also cases where poor lumbopelvic control can drive compensatory patterns in the thorax. Thus it is a combination of clinical tests, and not just one test, that leads to a clinical diagnosis of 'thorax-driven pelvic girdle pain/dysfunction'. The AsLR is one of the tests that helps build the clinical picture.
Clearly, more science is needed to provide greater understanding of the mechanisms and interactions that we are observing in the clinic. studies are required to identify subgroups of patients with thorax pain according to specific impairments, recognising that all patients do not have the same impairments, and to identify subgroups of patients with lumbopelvic and cervical pain that have a clinically relevant underlying thoracic impairment. Clinical tests for motion and load transfer need to be further developed and tested for reliability, validity, sensitivity and specificity. Through research at the CCRE in spinal Pain, Injury and Health at the university of Queensland, we are currently investigating the SAL test and other questions around muscle control and function in the thorax.
Specific ring palpation and correction during the ASLR.

In the meantime, based on the abundant literature on neuromuscular control in the rest of the spine combined with reflective clinical practice, we can build a model for effective approaches to the thorax that encompass not only increasing mobility, but also training control and creating optimal strategies for functional tasks. We have clinical tests that identify failed load transfer within the thorax, and then ways of testing specific systems (articular, neural, myofascial, and visceral) to determine which pieces of the clinical puzzle have impairments that are contributing to the non-optimal strategies and failed load transfer. We have other tests that assist in analysing when the thorax is a significant contributor and driver of pain in dysfunction in the shoulder girdle, neck, and lumbopelvic region. We have treatment techniques to address impairments in the different systems, including techniques to train and support inter-ring control. ultimately, restoration of optimal function requires stepping back and looking at the body as an integrated whole. This requires understanding not only the mobility requirements for tasks, but also analysing the load requirements, the level of predictability, and the threat value of the desired task. effective treatment programs are based around patient values and goals, and designed from specific assessment. This results in a multimodal approach that is patient-specific and tailored to meet the outcomes they deem important, and one that considers the biomechanical, neuro- muscular, and emotional needs of the patient.
So, at the end of the day, we can't ignore the thorax. We need to do more than mobilise or manipulate it - specific segmental analysis of movement strategies and control of this region is essential to effective outcomes for optimal function of our patients.
Linda-Joy Lee (BSc, BSc (PT), FCAMT, CGIMS, MCPA) is a Canadian Institutes of Health Research (CIHR) Fellow, clinical physiotherapist, and educator. She is known internationally for her skills in movement and performance analysis to restore optimum function and her integrated approach to treatment. 'LJ' has developed novel approaches to assess and train thoracic control in patients with spinal pain and dysfunction and is currently investigating these ideas in her PhD at the University of Queensland (Centre for Clinical Research Excellence in Spinal Pain, Injury and Health) under Paul Hodges and Michel Coppieters. She consults at her clinic, Synergy Physiotherapy, in North Vancouver, Canada, and teaches clinicians worldwide how to integrate multiple paradigms, new ideas and science for effective outcomes in clinical practice. Together with teaching partner Diane Lee, LJ is a founder of DiscoverPhysio, whose mission is to educate, inspire, and support clinicians worldwide in their professional journeys. For more information, visit: www.discoverphysio.ca and www.ljlee.ca. For a list of references, email: nsgeditor@physiotherapy.asn.au.



























.jpg)




















0 comentarios :
Publicar un comentario